Fill in a Valid Missouri Certificate Of Death Template
The Missouri Certificate of Death form is an essential document that serves multiple purposes in the event of a person's passing. This form captures vital information about the deceased, including their legal name, date of birth, and social security number. It also details the circumstances surrounding the death, such as the date and place of death, as well as the cause of death, which must be carefully documented by a certifying physician or medical examiner. The form requires information about the decedent's family, including the names of their parents and any surviving spouse, which can help in establishing identity and lineage. Additionally, the form includes sections for the informant's details, ensuring that the person providing the information can be contacted if needed. The method of disposition—whether through burial, cremation, or other means—is also recorded, along with the name and address of the funeral facility involved. This comprehensive approach ensures that all necessary details are captured, facilitating the legal and administrative processes that follow a death. Understanding the components of this form is crucial for those involved in managing the affairs of a deceased loved one, as it lays the groundwork for various legal and personal matters that must be addressed during a challenging time.
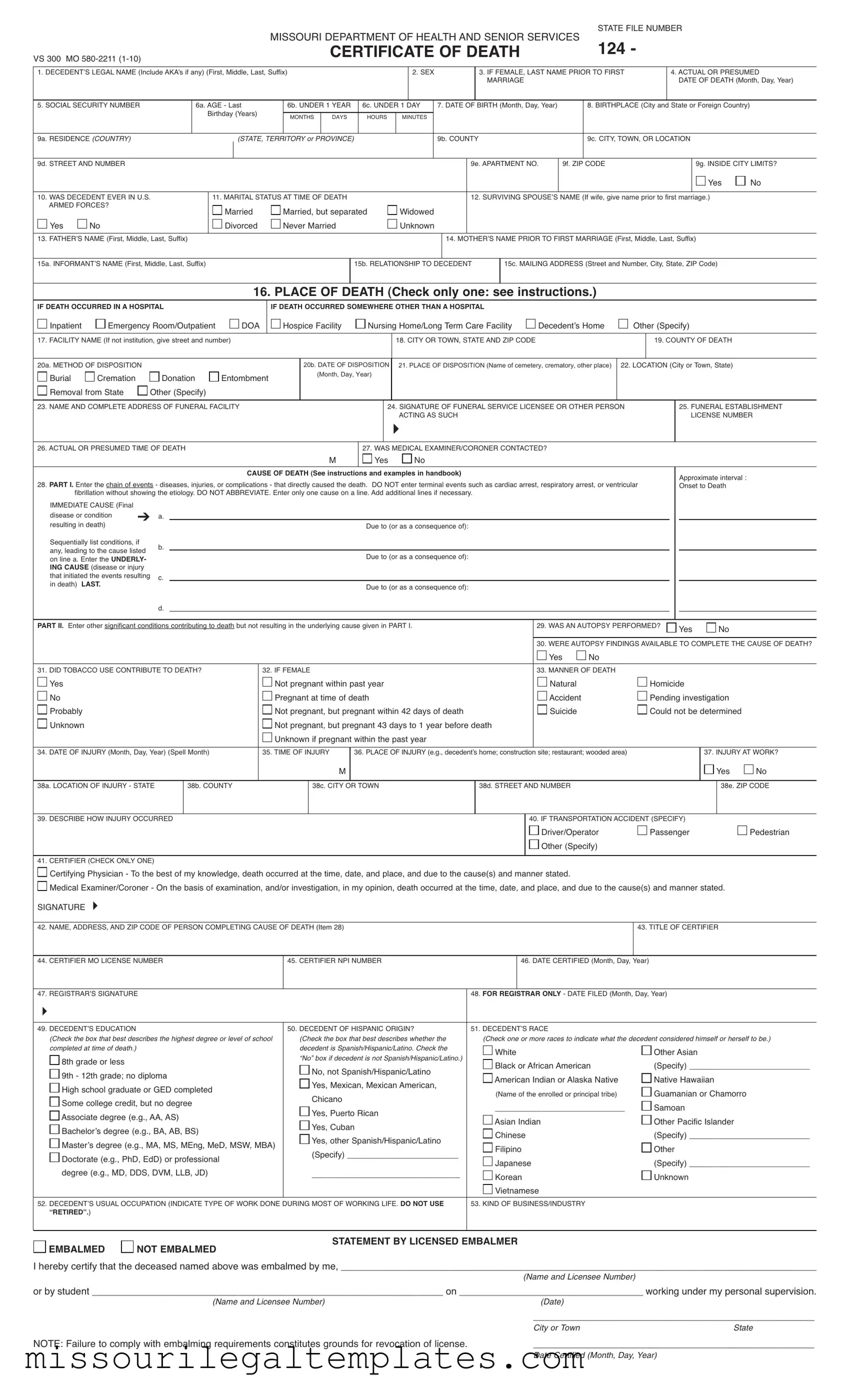
Missouri Certificate Of Death Preview
|
|
STATE FILE NUMBER |
|
MISSOURI DEPARTMENT OF HEALTH AND SENIOR SERVICES |
124 - |
VS 300 MO |
CERTIFICATE OF DEATH |
|
|
|
1. DECEDENTʼS LEGAL NAME (Include AKAʼs if any) (First, Middle, Last, Suffix)
2. SEX
3.IF FEMALE, LAST NAME PRIOR TO FIRST
3.MARRIAGE
4.ACTUAL OR PRESUMED
4.DATE OF DEATH (Month, Day, Year)
5. SOCIAL SECURITY NUMBER
6a. AGE - Last
6a. Birthday (Years)
6b. UNDER 1 YEAR |
6c. UNDER 1 DAY |
||
|
|
|
|
MONTHS |
DAYS |
HOURS |
MINUTES |
|
|
|
|
7. DATE OF BIRTH (Month, Day, Year)
8. BIRTHPLACE (City and State or Foreign Country)
9a. RESIDENCE (COUNTRY) |
(STATE, TERRITORY or PROVINCE) |
9b. COUNTY
9c. CITY, TOWN, OR LOCATION
9d. STREETAND NUMBER |
9e. APARTMENT NO. |
9f. ZIP CODE |
9g. INSIDE CITY LIMITS? |
|
|
|
|
Yes |
No |
|
|
|
|
||
10. WAS DECEDENT EVER IN U.S. |
11. MARITAL STATUS AT TIME OF DEATH |
12. SURVIVING SPOUSEʼS NAME (If wife, give name prior to first marriage.) |
|
||
10. ARMED FORCES? |
Married |
Married, but separated |
Widowed |
|
|
|
|
|
|||
Yes |
No |
Divorced |
Never Married |
Unknown |
|
|
|
|
|
|
|
13. FATHERʼS NAME (First, Middle, Last, Suffix)
14. MOTHERʼS NAME PRIOR TO FIRST MARRIAGE (First, Middle, Last, Suffix)
15a. INFORMANTʼS NAME (First, Middle, Last, Suffix)
15b. RELATIONSHIP TO DECEDENT
15c. MAILING ADDRESS (Street and Number, City, State, ZIP Code)
16. PLACE OF DEATH (Check only one: see instructions.)
IF DEATH OCCURRED IN A HOSPITAL
Inpatient |
Emergency Room/Outpatient |

 DOA
DOA
IF DEATH OCCURRED SOMEWHERE OTHER THAN A HOSPITAL |
|
|
|
Hospice Facility |
Nursing Home/Long Term Care Facility |
Decedentʼs Home |
Other (Specify) |
17. FACILITY NAME (If not institution, give street and number)
18. CITY OR TOWN, STATE AND ZIP CODE
19. COUNTY OF DEATH
20a. METHOD OF DISPOSITION |
|
|
|
Burial |
Cremation |
Donation |
Entombment |
Removal from State |
Other (Specify) |
|
|
20b. DATE OF DISPOSITION
(Month, Day, Year)
21. PLACE OF DISPOSITION (Name of cemetery, crematory, other place)
22. LOCATION (City or Town, State)
23. NAME AND COMPLETE ADDRESS OF FUNERAL FACILITY
24.SIGNATURE OF FUNERAL SERVICE LICENSEE OR OTHER PERSON
24.ACTING AS SUCH
�
25.FUNERAL ESTABLISHMENT
25.LICENSE NUMBER
26. ACTUAL OR PRESUMED TIME OF DEATH
M
27. WAS MEDICAL EXAMINER/CORONER CONTACTED?
Yes |
No |
CAUSE OF DEATH (See instructions and examples in handbook)
28.PART I. Enter the chain of events - diseases, injuries, or complications - that directly caused the death. DO NOT enter terminal events such as cardiac arrest, respiratory arrest, or ventricular fibrillation without showing the etiology. DO NOTABBREVIATE. Enter only one cause on a line. Add additional lines if necessary.
IMMEDIATE CAUSE (Final |
|
|
|
|
disease or condition |
➔ a. |
|
||
resulting in death) |
Due to (or as a consequence of): |
|||
|
|
|||
Sequentially list conditions, if |
b. |
|
||
any, leading to the cause listed |
|
|||
Due to (or as a consequence of): |
||||
on line a. Enter the UNDERLY- |
|
|||
|
|
|||
ING CAUSE (disease or injury |
|
|
||
that initiated the events resulting |
c. |
|||
in death) LAST. |
|
|
Due to (or as a consequence of): |
|
|
|
|
||
d.
Approximate interval : Onset to Death
PART II. Enter other significant conditions contributing to death but not resulting in the underlying cause given in PART I. |
29. WAS AN AUTOPSY PERFORMED? |
Yes |
No |
|
|||||
|
|
|
|
|
|
||||
|
|
|
|
30. WERE AUTOPSY FINDINGS AVAILABLE TO COMPLETE THE CAUSE OF DEATH? |
|||||
|
|
|
|
Yes |
No |
|
|
|
|
31. DID TOBACCO USE CONTRIBUTE TO DEATH? |
32. IF FEMALE |
|
|
33. MANNER OF DEATH |
|
|
|
|
|
Yes |
Not pregnant within past year |
Natural |
|
Homicide |
|
|
|||
No |
Pregnant at time of death |
Accident |
|
Pending investigation |
|
||||
Probably |
Not pregnant, but pregnant within 42 days of death |
Suicide |
|
Could not be determined |
|
||||
Unknown |
Not pregnant, but pregnant 43 days to 1 year before death |
|
|
|
|
|
|
||
|
Unknown if pregnant within the past year |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
||
34. DATE OF INJURY (Month, Day, Year) (Spell Month) |
35. TIME OF INJURY |
|
36. PLACE OF INJURY (e.g., decedentʼs home; construction site; restaurant; wooded area) |
|
|
37. INJURYAT WORK? |
|||
|
|
M |
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
38a. LOCATION OF INJURY - STATE
38b. COUNTY
38c. CITY OR TOWN
38d. STREETAND NUMBER
38e. ZIP CODE
39.DESCRIBE HOW INJURY OCCURRED
41.CERTIFIER (CHECK ONLY ONE)
40. IF TRANSPORTATION ACCIDENT (SPECIFY) |
|
|
Driver/Operator |
Passenger |
Pedestrian |
Other (Specify) |
|
|

 Certifying Physician - To the best of my knowledge, death occurred at the time, date, and place, and due to the cause(s) and manner stated.
Certifying Physician - To the best of my knowledge, death occurred at the time, date, and place, and due to the cause(s) and manner stated.

 Medical Examiner/Coroner - On the basis of examination, and/or investigation, in my opinion, death occurred at the time, date, and place, and due to the cause(s) and manner stated.
Medical Examiner/Coroner - On the basis of examination, and/or investigation, in my opinion, death occurred at the time, date, and place, and due to the cause(s) and manner stated.
SIGNATURE � |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
42. NAME, ADDRESS, AND ZIP CODE OF PERSON COMPLETING CAUSE OF DEATH (Item 28) |
|
|
43. TITLE OF CERTIFIER |
|||||
|
|
|
|
|
|
|
|
|
44. CERTIFIER MO LICENSE NUMBER |
45. CERTIFIER NPI NUMBER |
|
46. DATE CERTIFIED (Month, Day, Year) |
|||||
|
|
|
|
|
|
|
|
|
47. REGISTRARʼS SIGNATURE |
|
48. FOR REGISTRAR ONLY - DATE FILED (Month, Day, Year) |
||||||
� |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
49. DECEDENTʼS EDUCATION |
|
50. DECEDENT OF HISPANIC ORIGIN? |
51. DECEDENTʼS RACE |
|
||||
|
(Check the box that best describes the highest degree or level of school |
(Check the box that best describes whether the |
(Check one or more races to indicate what the decedent considered himself or herself to be.) |
|||||
|
completed at time of death.) |
|
decedent is Spanish/Hispanic/Latino. Check the |
White |
Other Asian |
|||
|
|
|
|
|
“No” box if decedent is not Spanish/Hispanic/Latino.) |
|||
|
8th grade or less |
|
|
|
|
|||
|
|
|
Black or African American |
(Specify) __________________________ |
||||
|
|
|
|
|
No, not Spanish/Hispanic/Latino |
|||
|
9th - 12th grade; no diploma |
|
|
|
||||
|
|
American Indian or Alaska Native |
Native Hawaiian |
|||||
|
|
|
|
|
Yes, Mexican, Mexican American, |
|||
|
High school graduate or GED completed |
|
|
|
||||
|
|
(Name of the enrolled or principal tribe) |
Guamanian or Chamorro |
|||||
|
|
|
|
|
Chicano |
|||
|
Some college credit, but no degree |
|
|
|
||||
|
|
____________________________ |
Samoan |
|||||
|
|
|
|
|
Yes, Puerto Rican |
|||
|
Associate degree (e.g., AA, AS) |
|
|
|
||||
|
|
Asian Indian |
Other Pacific Islander |
|||||
|
|
|
|
|
Yes, Cuban |
|||
|
Bachelorʼs degree (e.g., BA, AB, BS) |
|
|
|
||||
|
|
Chinese |
(Specify) __________________________ |
|||||
|
|
|
|
|
Yes, other Spanish/Hispanic/Latino |
|||
|
Masterʼs degree (e.g., MA, MS, MEng, MeD, MSW, MBA) |
|
|
|
||||
|
|
Filipino |
Other |
|||||
|
|
|
|
|
(Specify) ________________________ |
|||
|
Doctorate (e.g., PhD, EdD) or professional |
|
|
|
||||
|
|
Japanese |
(Specify) __________________________ |
|||||
|
|
|
|
|
|
|||
|
degree (e.g., MD, DDS, DVM, LLB, JD) |
________________________________ |
Korean |
Unknown |
||||
|
|
|
|
|
|
|||
|
|
|
|
|
|
Vietnamese |
|
|
52. DECEDENTʼS USUAL OCCUPATION (INDICATE TYPE OF WORK DONE DURING MOST OF WORKING LIFE. DO NOT USE |
53. KIND OF BUSINESS/INDUSTRY |
|
||||||
52. “RETIRED”.) |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
EMBALMED |
|
|
NOT EMBALMED |
STATEMENT BY LICENSED EMBALMER |
|
||
|
|
|
|
|||||
|
|
|
|
|
|
|
||
I hereby certify that the deceased named above was embalmed by me, ________________________________________________________________________________________
(Name and Licensee Number)
or by student _________________________________________________________________ on __________________________________ working under my personal supervision.
(Name and Licensee Number)(Date)
____________________________________________________
|
City or Town |
State |
NOTE: Failure to comply with embalming requirements constitutes grounds for revocation of license. |
____________________________________________________ |
|
Date Certified (Month, Day, Year)
Common PDF Templates
Missouri Mo Ptc - Utilizing this form responsibly can help residents maximize financial benefits provided by the state.
Why Sign Hipaa Privacy Form - It is important to understand your rights regarding your health information.
Dos and Don'ts
When filling out the Missouri Certificate of Death form, it is important to follow specific guidelines to ensure accuracy and compliance. Below is a list of things to do and avoid during this process.
- Do: Include the decedent’s full legal name, including any aliases.
- Do: Provide accurate dates, including the date of birth and date of death.
- Do: Clearly indicate the place of death, specifying whether it was in a hospital, hospice, or another location.
- Do: List the cause of death in detail, following the guidelines provided in the form.
- Do: Ensure that the informant’s name and relationship to the decedent are clearly stated.
- Do: Double-check the information for accuracy before submission.
- Do: Sign and date the form where required, ensuring all necessary parties have completed their sections.
- Don’t: Use abbreviations or shorthand when describing the cause of death.
- Don’t: Omit any required information, as this may delay processing.
- Don’t: Provide incomplete addresses for the decedent or the informant.
- Don’t: Leave any sections blank unless specifically instructed to do so.
- Don’t: Forget to check the appropriate boxes for marital status and military service.
- Don’t: Submit the form without ensuring that all signatures are present.
- Don’t: Attempt to alter any information after the form has been signed; corrections should follow the proper procedures.
Key takeaways
Ensure accurate information is provided for the decedent’s legal name, including any aliases. This is crucial for official records.
Fill out the date of death and date of birth accurately. These dates are essential for legal and statistical purposes.
Identify the place of death clearly. Indicate whether it occurred in a hospital, hospice, nursing home, or at home.
Complete the cause of death section with detailed information. List the chain of events that led to death, avoiding abbreviations.
Check the appropriate box for the manner of death. This can include natural causes, accidents, or other classifications.
Provide the informant’s name and relationship to the decedent. This helps verify the information provided on the form.
Misconceptions
Misconceptions about the Missouri Certificate of Death form can lead to confusion during an already difficult time. Here are four common misunderstandings:
- All information is optional. Many believe that they can skip certain sections of the form. However, providing complete and accurate information is essential. Each section serves a purpose, whether for legal, medical, or statistical reasons.
- Only the physician can fill out the cause of death. While the certifying physician is responsible for the cause of death, the informant—often a family member—must provide other critical details. This includes personal information about the decedent and circumstances surrounding the death.
- The form must be filled out immediately after death. Some think that the certificate must be completed within hours of death. In reality, there is a specific timeframe for filing, which allows for the necessary information to be gathered accurately.
- It is not necessary to report the decedent's education level. Some individuals may overlook this section, thinking it irrelevant. However, education data is important for public health statistics and can influence future health initiatives.
Understanding these misconceptions can help ensure that the Missouri Certificate of Death form is completed correctly and efficiently, ultimately easing the process for everyone involved.
Similar forms
The Missouri Certificate of Death form serves a vital role in documenting the details surrounding a person's death. Several other documents share similarities with this form, each serving specific purposes in the context of death and legal matters. Here are six documents that are similar to the Missouri Certificate of Death:
- Death Certificate: This is a general term for a document issued by a governmental authority that confirms a person's death. Like the Missouri Certificate of Death, it includes essential information such as the deceased's name, date of birth, date of death, and cause of death.
- Medical Examiner's Report: This document provides detailed findings from an autopsy or investigation conducted by a medical examiner. It often includes the cause of death and circumstances surrounding it, similar to the cause of death section in the Missouri Certificate of Death.
- Funeral Home Contract: This document outlines the services provided by a funeral home. It typically includes details about the deceased, similar to the information collected in the Certificate of Death, such as name, date of birth, and disposition method.
- Obituary: An obituary is a notice of a person's death, often published in newspapers or online. It usually contains biographical information about the deceased, including their name, date of birth, and date of death, much like the details found on the Certificate of Death.
- Will: A will is a legal document that outlines how a person's assets will be distributed after their death. While it does not directly relate to the cause of death, it often includes personal information about the deceased, similar to what is required on the Certificate of Death.
- Life Insurance Claim Form: This document is submitted to an insurance company to claim benefits after a policyholder's death. It typically requires a death certificate and information about the deceased, paralleling the details collected on the Certificate of Death.