Fill in a Valid Missouri Hipaa Template
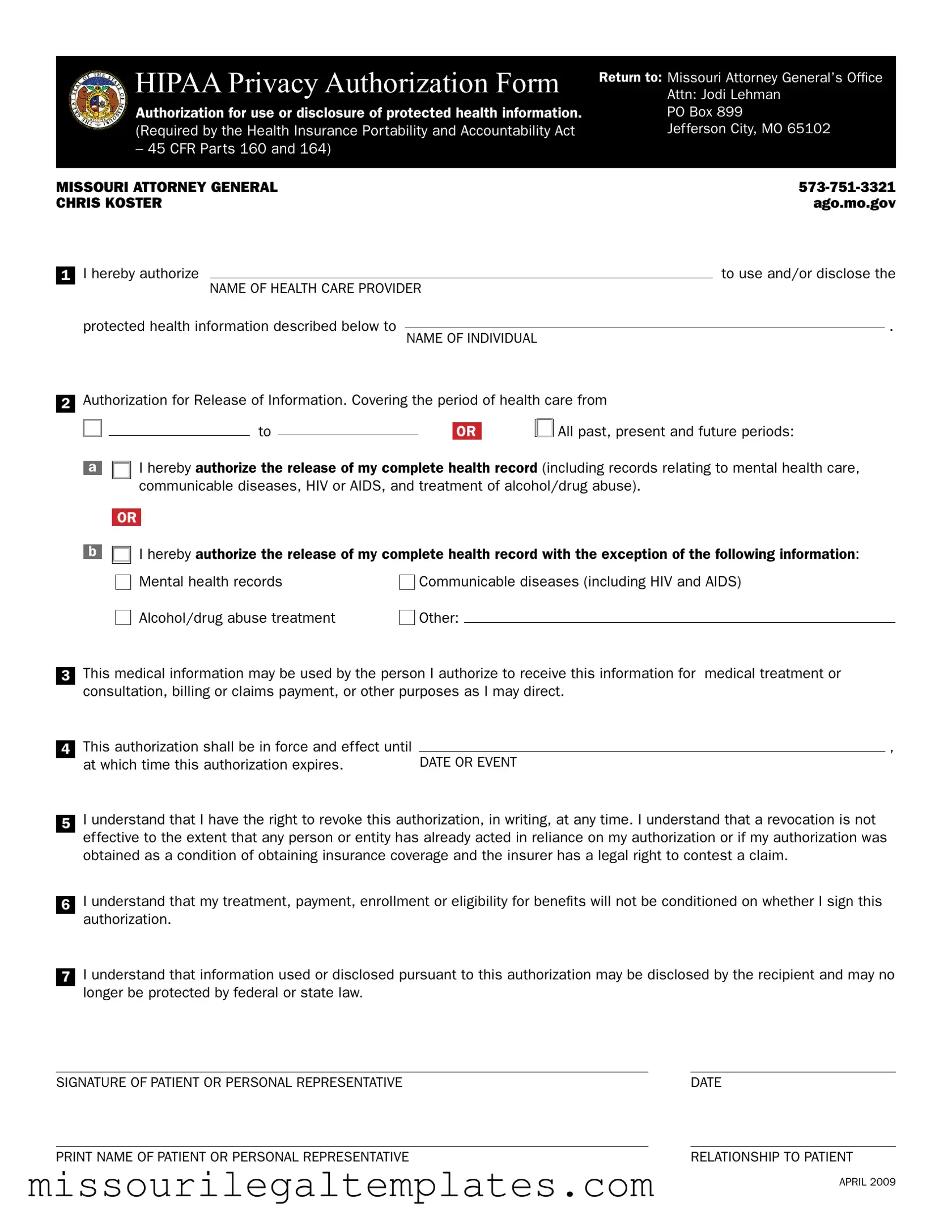
The Missouri HIPAA form is an essential document that allows individuals to authorize the use and disclosure of their protected health information. This form is a requirement under the Health Insurance Portability and Accountability Act (HIPAA) and is designed to ensure that patients have control over their medical records. It includes sections where individuals can specify the health care provider authorized to share their information and the person or entity that will receive it. Patients can choose to release their complete health record or limit the disclosure to specific types of information, such as mental health records or treatment for substance abuse. The form also outlines the duration of the authorization, allowing patients to determine how long their information can be shared. Importantly, individuals have the right to revoke their authorization at any time, although this revocation will not affect actions already taken based on the authorization. Understanding the implications of this form is crucial for anyone looking to manage their health information effectively.
Missouri Hipaa Preview















 HIPAA Privacy Authorization Form
HIPAA Privacy Authorization Form
Authorization for use or disclosure of protected health information. (Required by the Health Insurance Portability and Accountability Act
– 45 CFR Parts 160 and 164)
Return to: Missouri Attorney General’s Office Attn: Jodi Lehman
PO Box 899
Jefferson City, MO 65102
MISSOURI ATTORNEY GENERAL |
|
CHRIS KOSTER |
AGO.MO.GOV |
1
I hereby authorize |
|
|
to use and/or disclose the |
|
|
|
|||
NAME OF HEALTH CARE PROVIDER |
|
|
||
protected health information described below to |
|
|
. |
|
NAME OF INDIVIDUAL |
|
|||
|
|
|
|
|
2
Authorization for Release of Information. Covering the period of health care from
to |
|
|
OR |
All past, present and future periods: |
|
||||
|
|
|
|
|
a |
|
I hereby authorize the release of my complete health record (including records relating to mental health care, |
|||
|
|
communicable diseases, HIV or AIDS, and treatment of alcohol/drug abuse). |
|||
|
|
|
|
|
|
|
|
OR |
|
|
|
|
|
|
|||
b |
|
I hereby authorize the release of my complete health record with the exception of the following information: |
|||
|
|||||
|
|
Mental health records |
Communicable diseases (including HIV and AIDS) |
||
|
|
Alcohol/drug abuse treatment |
Other: |
|
|
|
|
|
|||
3
4
5
6
7
This medical information may be used by the person I authorize to receive this information for medical treatment or consultation, billing or claims payment, or other purposes as I may direct.
This authorization shall be in force and effect until |
|
, |
at which time this authorization expires. |
DATE OR EVENT |
|
I understand that I have the right to revoke this authorization, in writing, at any time. I understand that a revocation is not effective to the extent that any person or entity has already acted in reliance on my authorization or if my authorization was obtained as a condition of obtaining insurance coverage and the insurer has a legal right to contest a claim.
I understand that my treatment, payment, enrollment or eligibility for benefits will not be conditioned on whether I sign this authorization.
I understand that information used or disclosed pursuant to this authorization may be disclosed by the recipient and may no longer be protected by federal or state law.
SIGNATURE OF PATIENT OR PERSONAL REPRESENTATIVE |
DATE |
PRINT NAME OF PATIENT OR PERSONAL REPRESENTATIVE |
RELATIONSHIP TO PATIENT |
APRIL 2009
Common PDF Templates
Dmh 69 Missouri - The Dmh 69 form includes sections that ensure thorough assessments of programs.
For those looking to navigate the process smoothly, a reliable resource for the ATV Bill of Sale can be found at the following link. This document is vital for ensuring that the transfer of ownership and transaction details are accurately documented, safeguarding the interests of both involved parties. Access the important ATV Bill of Sale information here for your reference.
What Age Can a Child Choose Which Parent to Live With in Missouri - The petitioner must confirm their financial situation regarding the ability to pay for legal representation.
Dos and Don'ts
When filling out the Missouri HIPAA form, it's essential to follow certain guidelines to ensure accuracy and compliance. Here are six things to keep in mind:
- Do: Clearly write the name of the health care provider you are authorizing to disclose your information.
- Do: Specify the time frame for which you are authorizing the release of your health records.
- Do: Indicate whether you authorize the release of your complete health record or specify exceptions.
- Do: Sign and date the form to validate your authorization.
- Don't: Leave any sections blank; incomplete forms may delay processing.
- Don't: Forget to include your relationship to the patient if you are signing on someone else's behalf.
Key takeaways
Here are some key takeaways about filling out and using the Missouri HIPAA form:
- Authorization Requirement: You must provide clear authorization for a healthcare provider to use or disclose your protected health information.
- Specific Information: Be specific about what health information you are authorizing to be shared, including any exceptions for sensitive records.
- Duration of Authorization: The authorization remains valid until a specified date or event, after which it will expire.
- Revocation Rights: You have the right to revoke the authorization at any time in writing, but this does not affect actions taken before the revocation.
- Disclosure Risks: Be aware that once your information is disclosed, it may no longer be protected by HIPAA or state laws.
Misconceptions
Here are four common misconceptions about the Missouri HIPAA form:
- Misconception 1: Signing the form is mandatory for all medical treatments.
- Misconception 2: The authorization lasts indefinitely.
- Misconception 3: You cannot revoke the authorization once it is signed.
- Misconception 4: All health information is automatically protected after signing the form.
This is not true. You are not required to sign the HIPAA authorization form to receive medical treatment. Your healthcare provider cannot condition your treatment on signing this form.
The authorization does not last forever. It is valid only until the specified expiration date or event. After that, it is no longer effective.
You have the right to revoke your authorization at any time, in writing. However, if someone has already acted based on your authorization, that action remains valid.
Once you authorize the release of your information, it may be disclosed by the recipient. This means it might not be protected by HIPAA after being shared.
Similar forms
The Missouri HIPAA form is designed to authorize the use and disclosure of protected health information. This document shares similarities with several other forms related to health information privacy and consent. Below is a list of seven documents that are comparable to the Missouri HIPAA form, along with an explanation of how they are alike.
- HIPAA Release Form: Like the Missouri HIPAA form, this document allows individuals to authorize healthcare providers to share their health information with specified parties. Both forms ensure that patients have control over who can access their sensitive data.
- Patient Authorization for Disclosure of Health Information: This form is similar in that it grants permission for healthcare entities to disclose a patient's medical records. Both documents emphasize the importance of patient consent in the sharing of health information.
- Medical Records Release Form: This document serves a similar purpose by allowing patients to request their medical records from healthcare providers. Both forms facilitate the transfer of health information while ensuring patient rights are upheld.
- Informed Consent Form: While typically used for medical procedures, this form also requires patient authorization. Both the informed consent and the Missouri HIPAA form prioritize the patient's understanding and agreement before sharing health-related information.
- Authorization for Use of Health Information in Research: This form permits the use of health information for research purposes. Like the Missouri HIPAA form, it requires patient consent and outlines the specific information being shared.
- Power of Attorney for Healthcare: This document allows a designated person to make healthcare decisions on behalf of a patient. Both forms involve granting authority to another party regarding health-related matters, although the scope may differ.
- Florida Bill of Sale Form: Essential for legal transfer of ownership, this document protects buyers by providing proof of purchase and terms of sale, making it a vital tool for smooth transactions. For more details, visit TopTemplates.info.
- Release of Information for Insurance Purposes: Similar to the Missouri HIPAA form, this document allows for the disclosure of health information to insurance companies for claims processing. Both emphasize the necessity of patient authorization before any information can be shared.
Understanding these documents can empower individuals to make informed decisions about their health information and who has access to it. Each form plays a crucial role in protecting patient privacy while facilitating necessary communication within the healthcare system.